IMPLANTATION OF ENDOCARDIAC
PACEMAKER WITH ATRIAL LOOP IN INFANTS AND CHILDREN
Revaluation of
first experiences set in their historical background: recognition of a little
known and never claimed merit of Italian medicine
FerruccioDe Bellis1, Angelo Solinas1,
Antonio Ciccaglioni1, Vincenzo Colloridi2,
Giuseppe Palma1, Benedetto Marino3
1: Cardiac Electrostimulation Center of the Rome
University “La Sapienza” (CESC)
2: Pediatric Cardiology Institute of the Rome
University “La Sapienza”
3: Cardiosurgery Institute
of the Rome University “La Sapienza”
Summary
After some 50 years
of experience in the field of cardiac electrostimulation,
De Bellis, Palma and Ciccaglioni
with the important collaboration from Agostino Piro and Paolo Sonnino Silvani,
director of “Telemaco Software House” go back to the stages that 37 years ago (in
1976) led to the endocardiac pacemaker implantation in infants and children using
a new technique set up by the Authors that proved to be highly reliable, the
so-called “atrial loop”.
Herewith are presented
the clinical cases of endocardic implantations carried out for the first time
world-wide with the new simple, reliable and little-invasive technique that
assures a good quality of life to the small patients and consequently greatly increases
the PM indication in pediatric age.
In particular, it
is described the first of the interventions carried out with the new technique
in November 1976 on a patient of only 4 years of age.
Difficulties and
perplexities that had to be overcome are highlighted keeping in mind the
equipment available and the state of the art of ultrasonic diagnostics (Ecocardio).
Following the
arrival of the fixed-screw electrode in 1979, the Authors describe the
interventions carried out with the improved “atrial loop” technique as to
render the endocardiac implantation in infants and children less invasive and
more reliable.
State of art of
cardiac electrostimulation in 1976
Until 1976 PM implantations
in infants and children were carried out exclusively with thoracotomy and
epimiocardiac electrodes, without regard to age and body weight of the little
patients.
As known, the
bodily growth, in accordance to Godin’s Law, creates a discrepancy between the
size of thorax, the cardiac volume and the length of the stimulating electrode,
thus causing a noticeable and progressive tension of the electrode between the
tissue of the PM pocket and the anchoring on the epicardium, with high
probabilities of fractures and loss of stimulation.
In the specialized literature
several methods to overcome this complication were described, both for
endocardiac and epimiocardiac implant (electrode-catheter wound on a spool or
in a bag) but the results were practically of no value.
Furthermore, PM
implantation using thoracotomy on such young patients was extremely invasive
and burdensome.
The endocardiac
implantation, on the other hand, would have noticeably reduced the gravity of
the operation but the problems likewise would still be present.
In fact, between
the tissue of the pocket and the anchoring of the electrode-catheter in the
right ventricle, a noticeable and progressive tension would be created with consequent
risk of fractures and loss of stimulation.
It must be remembered
that at that time the technological progress of both PMs and electrode-catheter
was very limited. For instance, electrode-catheters were less flexible and
would easily dislocate within the three days following the operation.
PMs were
asynchronous or demand, programmable for only one or two parameters (frequency
and duration of the pulse), weighed 180 g and were 18 mm thick.
Ultrasonic
echocardiographic diagnostics was in its first phase.
An accurate
analysis carried out in 1981 and published in 1982 by the expert, Claudio Chiocchio,
was drawing this conclusion:
“At present stage of knowledge, the ultrasonic
equipment for diagnostic purposes implies no risk to the patient. It is
therefore probable that in the future, thanks to the undeniable advantages of
such technique and to the advancing progress of the technology of ultrasounds, the
latter could in certain cases replace invasive examination methods or
techniques using ionizing radiations. Until then, the method has to be
considered propaedeutic and complementary, especially for examination
techniques that do not entail the same advantages. In reality in this field
ultrasounds give very meaningful results but only the integration with other
methods would allow avoiding glaring blunders. The teaching gathered from
experience shows that before being an expert in echocardiography it is
important to be an expert cardiologist and have a good stethoscope.”
The new technique
In 1976 the Authors
perfected a technique to utilize the endocardiac stimulation also in pediatric patients.
The simple but
brilliant innovation, that will open the way to endocardiac stimulation for
pediatric ages, was that of introducing directly in the right atrium an excess length
of electrode-catheter, in order to compensate natural bodily growth, and to
accommodate the remaining electrode-catheter in the PM pocket.
It is evident that
the electrode in excess would be limited by the necessity to stabilize the
stimulating tip in order to avoid dislodgement and loss of stimulation.
It would not be
possible to insert immediately the approximately 30 cm of electrode-catheter
that would be required to compensate bodily growth for at least 3 or 4 years to
arrive at the time of first PM replacement.
Therefore, the
technique would require a second operation after about 8-10 months to insert in
the right atrium about 36 cm of electrode-catheter or whatever length was deemed
suitable to the weight, dimensions and expected growth of the child.
This technique was
immediately opposed by the cardiologists arguing that the ample curve of
electrode-catheter at first implantation and moreover the insertion of about 36
cm of electrode-catheter in the right atrium and in the inferior cava vein
during the operation at the eighth month, would cause thrombosis and embolism,
highly dangerous for the life of the young patients.
Moreover it was
feared that the ample curves of the electrode-catheter pushed against the right
atrium wall would create some fibrotic tissue capable to anchor the electrode-catheter
to the atrium wall thus preventing the un-winding of the stretch of the electrode-catheter
needed to compensate the bodily growth and to avoid the progressive tension
between the anchoring points, i.e. the tissue of the PM pocket and the wall of the
right ventricle, thus causing fracture and loss of stimulation.
The other thesis,
that eventually prevailed, implied that it would actually be the growth of the
patient and the movements of the cardiac muscle that would have prevented the
formation of adhesions and the creation of thrombosis and emboli.
Hence it was
decided to carry on with the implementation of the new technique on a young
patient that, due to the lengthy studies and discussions, had been waiting for
an operation for about 3 months.
The appropriateness
of such decision is confirmed in a study carried out by Vincezo Colloridi and
published by PACE in 1985 (“Ventricular Thrombosis during Permanent Endocardial
Pacing in a Pediatric Patient with Hemorrheological Disorder”) where it is
evidenced that the presence of thrombosis or emboli in patients of pediatric
age carrying endocardic PM is practically non-existent unless severe hemorrheological dysfunctions are present.
The first endocardiac implantation
On 13 December
1976, the first patient to have a PM implanted in accordance with the described
technique was Tonia C., a girl of 4, with a diagnosis of congenital TAVB (total
atrioventricular block) and congenital pulmonary stenosis (though minor and not
necessitating surgical treatment), subject to episodes of lipothymia.
The operation
consisted of surgical preparation of the right cephalic vein, insertion of the
electrode-catheter in the vein, guiding it against the right ventricular wall
and pushed until forming a wide and gentle curve in the right atrium.
The
electrode-catheter was anchored to the tissue with ligature on the vein.
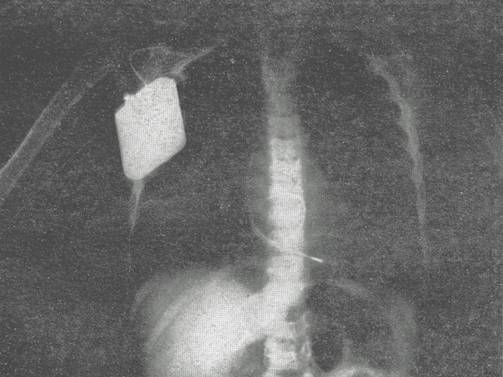
The remaining stretch of the electrode-catheter,
gently wound on itself, was accommodated below PM SP (single-chamber,
programmable with two parameters pacemaker) in a retromammary pocket above the
pectoralis major muscle.
Figure 1 shows the
position taken by the electrode-catheter.
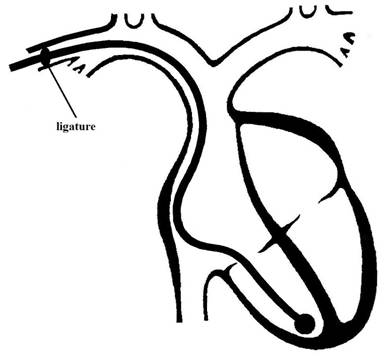
Figure 1
After dismissal of
the perfectly recovered patient on the seventh day, regular checks were carried
out every 3 months always controlling, by teleheart and X-ray, the curve of the
electrode-catheter in the right atrium.
The bodily growth
of the patient both in weight (from 15 kg to 18.8 kg) and in height (from 102
cm to 112 cm) and the configuration assumed by the curve of the
electrode-catheter in atrium led to the decision of performing a second operation
on 20 October 1977, as expected.
Figure 2 shows the
configuration of the electrode-catheter after 8 months with respect to the
original position.
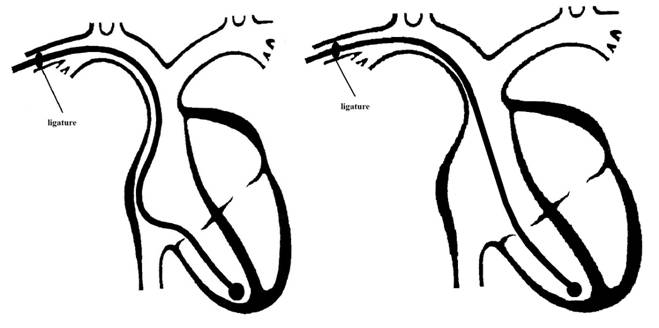
Figure 2
The following
procedure was used: open the PM pocket, free electrode-catheter from adhesions
and remove the ligature on the vein. Thanks to the then stable anchoring of the
stimulating tip to the right ventricular wall, it was possible to insert in the
superior cava vein about 30 cm of electrode-catheter in order to form an ample
curve in right atrium and a “U” curve in the inferior cava vein, as shown in
Figure 3.
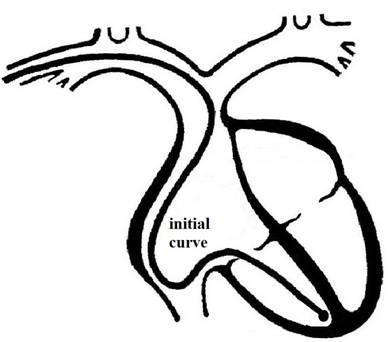
Figure 3
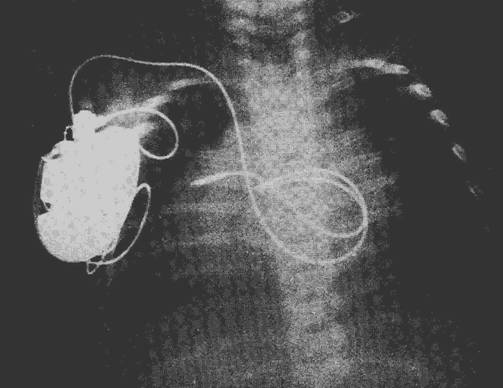
Having established
the ligature on the vein, the X-ray check showed that the ample curve in the atrium
and the “U” curve in inferior cava vein had disappeared
and the electrode-catheter had wound on itself at 360° to form a “loop” as
shown in Figure 4.
From this very
moment, the intervention to implant an endocardiac PM in infants and children was
indicated in specialized literature as “Endocardiac
Implantation with Atrial Loop”.
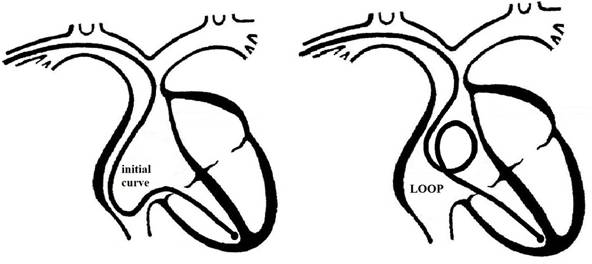
Figure 4
The patient was dismissed
perfectly healed on the seventh day; electronic and clinical tests of the PM were
performed at 6 month intervals.
At the electronic
check in April 1980, it was detected that the battery was in the second phase of
its life and hence the checks were performed at 3 month intervals.
On 5 February 1981 the
PM SP was replaced for low battery charge and a PM SM (pacemaker single
chamber, multiprogrammable) was implanted.
The X-ray
examination showed that the atrial “loop” had been replaced by a satisfactory
atrial curve; therefore the electrode-catheter was left in place, unmodified.
On 22 May 1986 a
new PM replacement operation was carried out and a new PM SR (pacemaker single
chamber, multiprogrammable, telemetric with sensor to vary cardiac rate) was
implanted.
The position of the
electrode-catheter, as seen by X-ray, was deemed satisfactory and therefore
left unmodified.
On 20 May 1990,
during a new PM replacement intervention, some more length of
electrode-catheter, to bring the total to 39 cm, was inserted. A PM SR was implanted.
On 25 March 1994 the
patient underwent a new intervention with transformation of the PM implant from
single chamber to dual chamber. The following method was used: puncturing of
the right subclavian vein with Seldinger technique, positioning of two fixed
screw electrode-catheter, one in right atrium and the other in right ventricle.
The old electrode-catheter was removed by simple constant pulling. A PM DR
(pacemaker dual chamber, multiprogrammable, telemetric with sensor) was implanted.
On 23 May 2001, at
the Cardiac Electrostimulation Center of the “Sapienza” University of Rome (CESC),
the last control of the patient’s PM was performed; on that occasion it was
decided that, for logistic reasons, it would be appropriate to perform future
controls in the patient’s town of residence.
On 28 November 2012
the patient was interviewed by telephone by a doctor from CESC; she declared a
state of well-being and confirmed that she regularly continues the checks in
the town where she lives.
The modified “atrial loop” technique
In 1979 the first fixed-screw
electrode-catheters became available; they would allow the safe and sure
anchoring of the electrode-catheter to the endocardium by means of the screw on
its tip. There were several advantages with this type of electrode-catheter:
1. Sensible reduction
of repositioning interventions of the electrode-catheter because of
micro-displacements that would cause non-tolerable increase of the cardiac
stimulation threshold (current needed to stimulate the heart);
2. Elimination of
displacements of the electrode-catheter, i.e. loss of contact with the
endocardium;
3. Easiness of removal
by “unscrewing traction” in case of infection;
4. Patients to be immobilized
for only 24 hours, a very important factor with respect to older and younger
patients.
On the other hand,
initially there were some disadvantages:
1. The screw tip would
often get caught on the inside of the vein thus creating serious problems to
the operator;
2. High cardiac
stimulation thresholds during the operation.
Those problems were
solved by:
1. Introduction of the
electrode-catheter in the vein by constant anti-clockwise rotation during advancement;
2. Screwing the
electrode-catheter tip to the endocardium with three clockwise turns while
exerting a gentle pressure.
3. Intra-operatory measurements
15 minutes after completion of the screwing.
The utilization of
the fixed-screw electrode-catheter for the “atrial loop" intervention has greatly
improved the technique as it allows to insert directly, during the first
implantation, the length of electrode-catheter deemed appropriate to the weight,
dimensions and expected growth of the infant or child.
Normally, a length
of 25 to 35 cm of electrode-catheter is inserted in the superior cava vein.
With this new
methodology it is possible to comply with the bodily growth without need for
the second intervention after about 8 months.
Besides, the
positive anchoring of the screw eliminates the stressful engagement of medical
and para-medical staff needed to keep the child immobilized during the first 3
or 4 days to allow the physiological anchoring of the electrode-catheter tip to
the endocardium.
This modified
technique, utilized by the Authors for the first time in the world in 1982, has
become the ELECTIVE UNIVERSAL METHODOLOGY FOR ENDOCARDIAC IMPLANTATION IN
INFANTS AND CHILDREN, the so called “Atrial
Loop Technique”.
First endocardiac
intervention with fixed screw electrode
On 16 January 1982,
Marco M. aged 4, with a diagnosis of congenital TAVB, was operated with the new
modified methodology, using for the first time a fixed-screw electrode-catheter.
The operation was
performed with the following procedure: right sub-clavian incision, located the
right cephalic vein, phlebotomy, insertion of the fixed-screw electrode-catheter
with a slow and constant anti-clockwise rotation to screw the tip of the
electrode-catheter to the endocardium of the right ventricle. Intra-operatory
measurements. Through the superior cava vein 32 cm of electrode-catheter were
inserted to form an ample curve in right atrium and a “U” curve in the inferior
cava vein. Ligature of the electrode-catheter on the vein, right subcutaneous
pocket, layered suture. Electrode-catheter connected to a PM SM.
The X-ray taken in
the operating theater after the intervention shows the “loop” formed by the 32
cm of electrode-catheter inserted in the right atrium.
On 22 July 1988, after
well over 6 years, the PM SM was replaced with another PM SM. On that occasion a
further stretch of electrode-catheter was inserted through the superior cava
vein, for a total of 39 cm, in order to form a slightly wider “loop”.
On 12 September
1991, during a normal electronic check of the PM, the X-ray was still showing
the presence of the “loop” in right atrium.
On 16 July1993 the
implant was transformed with the following procedure: puncturing the right
subclavian vein with Seldinger’s method, insertion of atrial fixed-screw electrode-catheter
and anchoring it in appropriate position, intra-operatory measurements. The
X-ray showed the disappearance of the “loop” transformed into a wide curve in
atrium. The ventricular electrode-catheter had been left untouched. Electronic
check of the PM SM at 6 month intervals.
On 3 May 2001, after
an early check, it was decided to replace the PM because the battery was
approaching discharge. Taking into account the tests carried out at the regular
checks of the PM, the patient was included in the operatory list for: New PM
implantation.
On 8 June 2001 the
new PM implantation took place with the following procedure: right sub-clavian
incision to find the right cephalic vein; double phlebotomy. Separated
ligatures, the proximal for the atrial electrode-catheter, the distal for the
ventricular electrode-catheter. Unipolar electrode-catheter with barbs in right
ventricle, unipolar “J” pre-formed electrode-catheter with barbs in right
atrium.
Connected the PM DR
to the electrode-catheters and positioned it in a left subcutaneous pocket. Open
the right subcutaneous pocket it was attempted to extract the two pre-existing electrode-catheters
that got stuck and were left there fixed to the subcutaneous layer with
ligature on silicone tubes.
On 2 May 2011 the PM
DR was replaced.
As of 28 November
2012, the patient regularly follows the PM electronic checks at the Cardiac
Electrostimulation Center of the “Sapienza” Università of Roma (CESC).
The first endocardiac intervention on an infant with “atrial loop”
technique
On 21 March 1982 the
2-months old infant Stefania D. G was admitted to
CESC with a diagnosis of situs inversus viscerum (inverted position of internal
organs), severe pulmonary hypertension and severe bradicardia (40-60 bpm).
The very young age
of the patient required the surgical preparation of the right sub-clavian vein. When a branch of adequate caliper was found,
a phlebotomy was performed through which the fixed-screw electrode-catheter was
inserted with constant anti-clockwise rotation to screw it to the right atrium
endocardium.
The complex
congenital malformation made the insertion and the positioning of the fixed-screw
electrode-catheter particularly difficult and it was necessary to avail of a
ball catheter to detect with X-ray the atrium. Intra-operatory measurements. Through the superior cava vein 24 cm of
electrode-catheter were inserted. Anchored to the sub-cutaneous with double
silk ligature on the sub-clavian vein branch.
The X-ray taken
after the operation clearly shows the “atrial loop”.
The little patient
has been undergoing regular checks of the PM.
On 16 April 1986 the
PM SM was replaced with another PM SM and a total of 36 cm of
electrode-catheter were inserted to form a wider loop in atrium.
On 8 January 1987,
after a regular check of the PM, the relatives of the patient communicated the
decision to continue regular checks of the PM in the town of residence.
Conclusions
The experience
relates to 11 cases, 5 of which with electrode-catheter with spherical tip, with
or without lance, and 6 cases with fixed-screw electrode-catheter.
The age of the patients
varied between two months and 5 years. Five cases were post-surgical TAVB. Three
cases were congenital AVTB. The remaining cases have been described above in
details.
As stated before,
the “atrial loop” methodology first developed by the Authors, has become
worldwide the elective technique for implantations in infants and children,
also in case of post-surgical TAVB.
The experience of
the Authors ended after 1985 when the Roman hospitals’ specialized departments
were created also for this branch that would obviously avail of the “atrial
loop” technique.
These successful
results in cardiac electrostimulation in infants and children were presented:
-
Nationally, at
the 2nd National Congress on Cardiac Electrostimulation held in Rome, Italy, on
7th and 8th December 1978
-
Internationally, at the 7th World Symposium on Cardiac
Pacing, Vienna, 1st-5th May 1983.
Published on:
-
Giornale Italiano di Cardiologia, Acts of
II National Congress of Cardiac Electrostimulation,
Vol. VIII, Suppl. 3, 1978: “Pacemaker
Endocardico Permanente in Soggetti di Età Pediatrica”
-
Cardiologia – Bulletin
of the Italian Society of Cardiology – Volume XXVIII – Fasc. 4 –April 1983:
“Risultati di Sette Anni di Esperienza nell’Elettrostimolazione Cardiaca
Endocardica a Lungo Termine nei Neonati e nei Bambini”
-
Proceedings of the VIII World Symposium on Cardiac
Pacing and Electrophysiology, Abst.– 640, May 1983:
“Results of a seven-year experience in the long term electrostimulation in
infants and babies”
Comments
Benedetto Marino – Cardiosurgery Professor Emeritus –
“SAPIENZA” Rome University
A review of the 1978 work regarding implantation of a
pacemaker with atrial loop in 1976, lends a romantic air to a clinical
experience, the first in the world to resolve a problem in young children.
Rereading that work, there is a spontaneous
consideration regarding the working method of a group, that had been entrusted
by Prof. Pietro Valdoni
with the task of developing the cardiac electrostimulation,
a technique which was already spreading rapidly.
With farsighted vision, also a passionate and
brilliant bio-medical engineer (De Bellis) was
recruited in the team, which was rare at that time.
It was in fact the “passion” united with intelligence
that allowed the solution of numerous technical problems, the registration of
patents subsequently applied by the industry, or in this clinical case, the
“invention” of the atrial loop. Despite the amount of time that has elapsed,
this solution remains valid and still is in clinical use.
We said: passion, cleverness, dedication and, we wish
to add, cheerfulness in the work of a team that paid no attention to
organizational schemes, modularity, hierarchies or career aspirations.
We believe that these are and remain the fundamental
ingredients for innovation and development, short of saying: “Give me a brain
and a pencil and I’ll do the research”
There is no doubt that even now, when sophisticated
technological support and apportioned economic planning cannot be renounced,
INNOVATION and DEVELOPMENT cannot preclude a true and GENEROUSLY LIVED PASSION.
This small but meaningful scientific contribution of
fifty years ago is the witness
Benedetto
Marino
Prof.
Francesco Fedele – Director Cardiology Dept. –
“SAPIENZA” Rome University
The branch of cardiology
that in the last 50 years has undergone the fastest and most revolutionary
technological progress is the cardiac electrostimulation.
From the monocameral pacemakers that were used to
treat total atrio-ventricular blocks, lasting just a
few months, we have passed to the bi-cameral pacemakers to treat the atrial
sinus node disease and the atrio-ventricular blocks,
that presently have to be replaced after 6-10 years, and have arrived at the
treatment of heart failure with re-synchronization therapy.
For these reasons, as a
cardiologist always attentive to technological innovations in cardiology, I am
pleased to comment on this work.
During the aforementioned
evolution, especially in the first years, the few experts in the field had to
sharpen their wits in order to solve important problems with the technology
then available to them.
Keeping this in mind, we
relate the Authors’ experience when they firstly tackled the problem of
implanting a pacemaker in infants and children, in particular the most relevant
problem - that is the discrepancy created in time between bodily growth and
electrode-catheter length.
This event, already noticed
in epicardiac implants, would appear even more
pronounced in the first endocardiac implants with a
progressive tension of the electrode-catheter eventually leading to its
fracture.
To overcome the problem, the
little patients had to periodically undergo operations, according to their
growth, in order to push some length of the electrode-catheter that had been
left in the pacemaker pocket.
The Authors’ innovation was
to create, at atrial level, a loop of the ventricular electrode-catheter, in
order to allay the need for these interventions. In the first cases, when the
screw electrode-catheter was not yet available, the Authors would create the
loop after 6-8 months from the implant because it was necessary to wait for the
tip to become fixed to the ventricle by fibrotic tissue. When the screw
electrodes became commercially available, the problem was overcome as the
creation of the loop would not dislocate the electrode-catheter.
Still today, thanks to the
experiences gathered by the Authors, all interventions on small children are
performed with the atrial loop and, for sure in the near future with the coming
of the nano-technologies, this pioneering intuition
will be replaced by cardiac electrostimulation
without electrode-catheters.
At a time when there is a
tendency to consider the cardiologist at the mercy of a technology that more
and more heavily conditions any important clinical and therapeutic choices,
this “pioneering’ work” of a team of cardiologists, cardio-surgeons and
bio-engineers is an example of how technology does not have to be considered as
the divinity of our days, but can be reconsidered in a managerial and clinical
context that is more patient-oriented.
Francesco Fedele